 Home
Home
|
Table of Content Volume 16 Issue 3 - December 2020
Utility of 3.0 tesla diffusion tensor imaging and fibre tractography in neurological disorders
Shashank G D1, Ashwini Bahua2*
1Associate Professor, 2Senior Resident, Department of Radiology, Subbaiah Institute of Medical Sciences, Shimoga INDIA. Email: ash.bahua@gmail.com
Abstract Background: Diffusion tensor imaging (DTI) is a magnetic resonance (MR) imaging technique that can be used to characterize the orientational properties of the diffusion process of water molecules. It enables the measurement of the restricted diffusion of water in tissue in order to produce neural tract images. Usually, the information is contracted to two types of parameters: diffusion anisotropy, which represents the amount of directionality, and orientation of the axis along which water molecules move preferentially. Application of this technique to the brain has been demonstrated to provide exceptional information on white matter architecture. Objectives: To evaluate the role of diffusion tensor imaging and fibre tractography in demonstrating abnormalities in a variety of disorders in neurology ranging from multiple sclerosis to neurodegenerative disorders. Methodology: The study was performed after taking permission and due clearance from ethical committee and included selected patients who were referred for MRI examination from January 2017 till November 2018. Patients’ general clinical history and history pertaining to neurology, in particular, were noted and physical examination performed. Results: Majority of the patients were from 11-20 years age group i.e. 22% followed by 16% each from 0-10- and 41-50-years age group. 24 i.e. 48% were males and 26 i.e. 52% were females 15(30%) patients had headache as the chief complaint, 9(18%) patients had seizures as their chief presenting complaint, 6(12%) patients presented with visual disturbances, 1(2%) patient with hearing impairment, 4(8%) patients presented with altered sensorium, 1(2%) patient with cranial nerve deficits, 2(4%) patients with memory deficits, 8(16%) patients with fever and 2(4%) with cerebellar symptoms. 2(4%) patients were asymptomatic. Infectious and benign aetiology was detected in 9 patients each i.e. 18% followed by 8 i.e. 16% as congenital and developmental anomaly. Malignant aetiology was seen in 14% and infarct in 14% patients. Conclusion: Our study has proved that diffusion tensor imaging and fibre tractography, a state of the art technology‘ when used as an adjunct to conventional MRI sequences reveals a whole lot of information about the white matter and the white matter tracts. It is the only non-invasive investigation which can image the white matter tracts of central nervous system. Key Words: 3.0 tesla diffusion tensor imaging, fibre tractography, neurological disorders.
INTRODUCTION Imaging of central nervous system (CNS) involves imaging of brain and spine. Till recently, conventional magnetic resonance imaging (MRI), computed tomography (CT) scan and in infants, trans-cranial ultrasound (USG), were the primary modalities for imaging CNS. Diffusion MRI (or dMRI) is a magnetic resonance imaging (MRI) method which came into existence in the mid-1980s.1,2 It allows the in vivo mapping of the diffusion process of molecules, mainly water; in biological tissues, non-invasively. Molecular diffusion in tissues is not free, but reflects interactions with many obstacles, such as macromolecules, fibres, membranes, etc. Water molecule diffusion patterns can therefore reveal microscopic details about tissue architecture, either normal or in a diseased state. The first diffusion MRI images of the normal and diseased brain were made public in 1985.3 Since then, diffusion MRI has been extraordinarily successful. Its main clinical application has been in the study and treatment of neurological disorders, especially for the management of patients with acute stroke. Diffusion tensor imaging (DTI) is a magnetic resonance (MR) imaging technique that can be used to characterize the orientational properties of the diffusion process of water molecules. 4,5 It enables the measurement of the restricted diffusion of water in tissue in order to produce neural tract images. Usually, the information is contracted to two types of parameters: diffusion anisotropy, which represents the amount of directionality, and orientation of the axis along which water molecules move preferentially. Application of this technique to the brain has been demonstrated to provide exceptional information on white matter architecture.6, 7, 8, 9, 10 As at present there is no other imaging modality that can provide equivalent information, Diffusion tensor imaging is expected to become an important tool for the study of brain anatomy and the diagnosis of various white matter abnormalities.11 To evaluate the role of diffusion tensor imaging and fibre tractography in:
MATERIAL AND METHODS The study was performed after taking permission and due clearance from ethical committee and included selected patients who were referred for MRI examination from January 2017 till November 2018. Patients’ general clinical history and history pertaining to neurology, in particular, were noted and physical examination performed. Inclusion and exclusion criteria were reviewed. PATIENT DATA COLLECTION: The format used for data collection included:
INCLUSION CRITERIA:
EXCLUSION CRITERIA:
DATA ACQUISITION All patients were examined on a 3.0 T MR scanner (Philips MR Systems Achieva 3.0 T Release 2.6.3.5). DTI data were acquired using a single-shot echo planar imaging (EPI) sequence with parallel imaging (sensitivity Encoding factor, R = 2.5). The imaging matrix was 112 × 112 with a field of view of 246 × 246 mm (nominal resolution of 2.2 mm), which was zero filled to a 256 × 256 matrix. The image orientation was axial with 2.2 mm slice thickness, which was aligned parallel to the anterior–posterior commissure line. A total of 55 slices covered the entire cerebral hemispheres and the brainstem. The diffusion weighting was encoded along 15 independent orientations with maximum b = 800 mm2/s. Co-registered conventional clinical pulse sequences, including T1w (TR/TE500/27ms), T2w (TR/TE 4000/90ms), FLAIR (TR/TI/TE 6000/2000/120ms) in a combination of coronal, sagittal and axial planes with the same resolution were also recorded for anatomical guidance. Post contrast T1 images were also recorded in indicated cases. Advanced imaging techniques like MR Spectroscopy, MR Perfusion studies, MR CSF Flow studies were performed in indicated cases. Scanning time was 6min 12sec per DTI sequence and overall the imaging time was approximately 50 minutes for routine sequences but it varied and increased up to 2 hours as many other sequences were also needed for some patients and sometimes sequences had to be repeated and some patients needed general anaesthesia/sedation. DATA PROCESSING The DTI datasets were transferred to a workstation and processed. All diffusion weighted images were visually inspected for apparent artefacts due to subject motion and instrumental malfunction. Then, the 6 elements of the diffusion tensor were calculated for each pixel using multi-variant linear fitting. After diagonalization, three eigenvalues (λ1, λ2, λ3) and three eigenvectors (v1, v2, v3) were obtained. For the anisotropy map, the so-called fractional anisotropy (FA) parameter was calculated, which is scaled from 0 (isotropic) to 1 (anisotropic). The eigenvector associated with the largest eigenvalue was utilized as an indicator for the fibre orientation. In the colour map, red (R), green (G), and blue (B) colours were assigned to right-left, anterior-posterior, and superior-inferior orientations, respectively. For the colour presentation, a 24-bit colour scheme was used, in which each of RGB colours had an 8-bit (0–255) intensity level. In order to suppress orientation information in isotropic brain regions (there should not be a preferential orientation in isotropic areas and the calculated orientations in such areas are dominated by noise), the 24-bit colour value was multiplied by the FA value.
RESULTS
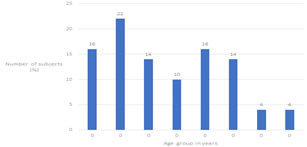
Figure 1: Distribution according to age group Majority of the patients were from 11-20 years age group i.e. 22% followed by 16% each from 0-10- and 41-50-years age group. 14% each were from 21-30 and 51-60 years age group.
Figure 2: Distribution according to gender In our study, 24 i.e. 48% were males and 26 i.e. 52% were females
Table 1: Distribution according to clinical presentation
Table 2: MRI detected findings
Infectious and benign aetiology was detected in 9 patients each i.e. 18% followed by 8 i.e. 16% as congenital and developmental anomaly. Malignant aetiology was seen in 14% and infarct in 14% patients. The diseases affecting the brain can be divided into congenital, neoplastic (including benign and malignant), infectious, seizure disorder, traumatic and post- operative. The congenital conditions that we came across during our study included corpus callosum agenesis, Dandy Walker malformation, persistent cavum pellucidum, heterotropia, arterio-venous malformation etc. Neoplastic conditions encountered included both benign and malignant conditions like meningioma, craniopharyngioma, epidermoid, low grade glioma, glioblastoma multiformae, astrocytoma, etc. and other space occupying lesions like dural cyst. Infectious diseases affecting the CNS included conditions like intracranial tuberculomas, neurocysticercosis, bacterial and viral meningitis, intracerebral abscess, subdural empyema etc. Seizure disorders included mesial temporal sclerosis and epileptic foci around glotic areas due to various causes. Intra-cerebral haemorrhage encountered in two patients was secondary to hypertension and hypoxic ischaemic encephalopathy. Infarcts in varying stages-acute, subacute and chronic were included and most of them were secondary to ischaemia due to age related atherosclerotic changes within the arteries whereas few of them were secondary to inflammatory conditions like aortoarteritis and infective conditions like tuberculosis. DISCUSSION Congenital and developmental anomalies Out of 50 patients, 9(18%) patients were detected to have various congenital and developmental anomalies of which 2(4%) patients had complete agenesis Of corpus callosum, 1(2%) patient had Dandy Walker malformation, 1(2%) patient had heterotropia, 1(2%) patient had non lissencephalic cortical dysplasia, 1(2%) patient had persistant cavum septum pellucidum, 2(4%) patients had neurofibromatosis with associated intra cerebral hamartomas and 1(2%) patient had an arterio-venous malformation. Once a congenital abnormality was suspected, further clinical, laboratory and imaging evaluation were performed to assess the neurological, cognitive and behavioural status of the patient. Early diagnosis of accompanying complications like hydrocephalus, papilloedema and cerebral herniations were made in order to prevent permanent neurological damage. Although most of the abnormalities like absent corpus callosum, heterotropias, large posterior fossa in Dandy Walker malformation etc were seen on conventional MRI sequences, DTI helped in better delineation and characterization of the abnormalities. In our study, analysis of the fractional anisotropy values within the unidentified bright objects in two patients with neurofibromatosis (NF) 1 showed no significant variation in comparison with the FA of the normal brain parenchyma. This is consistent with a study done by Van Engelen S. J. et al. who in their paper, Quantitative differentiation between healthy and disordered brain matter in patients with neurofibromatosis type I using diffusion tensor imaging‘, published in 2008 in American Journal of Neuroradiology, have also revealed no significant differences in fractional anisotropy values within the unidentified bright objects among 50 children with NF1 and 8 healthy controls.12 Hans-Joachim Mentzel et al. have also come up with the same inference. 13 NEOPLASTIC: In our study, 16(32%) patients had intracranial neoplasms out of which 5(10%) were primary malignancies, 2(4%) were metastasis, and 9(18%) were benign neoplasms. Among the malignant neoplastic lesions glioblastoma multiformae was most common, seen in 2(4%) patients. oligodendroglioma, brain stem glioma and sub ependymal gaint cell astrocytoma were seen in 1(2%) patients each respectively. Metastases were seen in 2(4%) patients, primary malignancy being melanoma in one patient and bronchogenic carcinoma in the other. Out of 9 patients with benign neoplasms, meningioma was most common, seen in 7(14%) patients. 1(2%) patient had right cerebellopontine angle epidermoid tumour and 1(2%) patient had a benign dural cyst arising from the anterior dura of the thoracic spinal canal. Few patients were evaluated with CT brain prior to our study. MRI brain with contrast was performed in all these patients. Extra sequences were performed whenever indicated. Conventional MR sequences provided adequate information about the location and size of the tumour. However, it did not provide much information on grade and invasiveness of the tumour and intra-tumoral diffusion characteristics. DTI was performed in a patient who presented with a solitary cerebral metastasis from malignant melanoma in the right foot. Region of interest (ROI) drawn within the tumour shows extremely low FA value. ROI drawn in the surrounding white matter shows decreased FA values with increased ADC values, in comparison with the ROI drawn in the corresponding region on contralateral side suggesting cerebral oedema rather than invasion. K Tsuchiya et al. have performed a study in 2005 to differentiate between solitary brain metastasis and high-grade glioma using diffusion tensor imaging. In conclusion, they stated that solitary brain metastases and high-grade gliomas could not be reliably differentiated either visually or quantitatively on the basis of FA changes. However, a diagnosis of brain metastasis was suggested when FA maps outline the tumour or when they demonstrate displacement of adjacent white matter fibres. They also opined that future improvements in spatial resolution might increase the diagnostic capability of FA maps in this regard. 14 INFARCTS: DTI was performed in 5 patients who presented with acute infarct belonging to varied age groups. It was observed that there was a decrease in FA value within the infarcted area in comparison to the corresponding normal white matter in the opposite cerebral hemisphere. In patients with chronic infarcts a decrease in the FA values of the white matter tracts arising from the infarcted area was observed denoting Wallerian degeneration. These findings were consistent with the study performed by David J Werring in 2000 which demonstrated reduced fibre anisotropy associated with cerebral infarction and also in the corticospinal tract remote from the lesion, in five patients 2 to 6 months after ischaemic stroke.15 Perinatal insults, including anoxia, may lead to a form of cerebral necrosis designated multicystic encephalomalacia. This common condition is characterized by moderate atrophic ventricular dilatation with intact ventricular walls with thickened subependymal glial layer and multiple cysts of irregular size and shape distributed throughout the cerebral white matter and the inner layers of the cortex bilaterally as described by Naidich T P et al..16 DTI was performed in a 35 year old male who came with cystic encephalomalacia involving the left temporal white matter. On analysing the DTI data, a diffuse loss of white matter fibre bulk was observed. There was gross alteration of FA map with decreased FA values within the involved white matter which showed altered signal intensity on conventional MR images.
CONCLUSION
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Radiology (Print ISSN: 2579-0927) (Online ISSN: 2636-4689) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
Height, IVDL-Intervertebral Disc Length
Policy for Articles with Open Access
Authors who publish with MedPulse International Journal of Radiology(Print ISSN: 2579-0927) (Online ISSN: 2636 - 4689) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work. |
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.