 Home
Home
|
Table of Content Volume 17 Issue 1 - Janaury 2021
Study of erectile dysfunction patients of flaccid penis using penile colour doppler sonography in Telangana population
Abhijith Kumar kotte1, Balaji Patel Kola2*
1Assistant professor, 2Associate Professor, Department of Radiology, Apollo Hospital, Apollo Institute of Medical Sciences and Research, Jubilee Hills, Hyderabad-500096, Telangana, INDIA.
Abstract Background: Erectile dysfunction (ED) is an inability to achieve and maintain erectile rigidity sufficient for satisfactory sexual performance. It is either organic or psychogenic. Hence, to differentiate and diagnose vasogenic study is evaluated. Method: 44 patients having ED were studied who had ED since the last six months. After examination in flaccid state, papaverine injected with grayscale and colour doppler sonography using ultrasound unit with a high-frequency wideband 6-13 MHz linear array transducer. The clinical response of intracavernous injection was also evaluated. Sensitivity, specificity, negative predictive values (NPV), Positive predictive values (PPV) of peak systolic velocity (PSV) in the flaccid and erect state were studied, PSV less than 25 (<250 cms/sec after papaverine injection is criteria for arterial insufficiency) is considered abnormal. Results: 11 (27.5%) patients were abnormal and 29 (72.5%) were normal with clinical response. At 10 minutes after papaverine injection sensitivity was 91.5% and specificity was 92.8 NPV was 96.8% and PPV was 80.9% Conclusion: Colour doppler is an ideal method to investigate vascular insufficiency of the penis in erectile dysfunction as a primary cause. Keywords: CC, corpora cavernosa, ED=erectile dysfunction, NPV, PPV, PCV, papaverine
INTRODUCTION Erectile dysfunction (ED) is defined as a consistent inability to achieve and maintain erectile rigidity sufficient for satisfactory sexual performance1,2. A complex mechanism is required to attain penile erection, involving synchronous and coordinated interaction of nervous, arterial, venous and sinusoidal systems. A disruption of any of these components usually results in ED. There are three corporal bodies in the penis two dorsally placed corpora cavernosa and single ventrally placed corpus spongiosum (CS), which contains the urethra. Three are enclosed in a bulk fascia and two CC are separated by a septum which has fenestrations that allow communications between corpora bodies, corporal arteries, internal pudendal arteries which arise from Internal Iliac arteries. The venous drainage of CC is by emissary vein which drains into dorsal crural and cavernous veins3,4. When the penis is flaccid its smooth muscle is in a tonic state the cavernous sinusoids collapse and the cavernous venules are open. Erection starts when an autonomic neurogenic impulse relaxes the cavernosal arterioles and sinusoidal spaces. Arterial inflow increases into the penis as the cavernous arteries dilate. This is accompanied by relaxation of the smooth muscle of CC with expansion and elongation of cavernous sinusoids then filled with blood. The venules and emissary veins are compressed against the taut tunica albuginea which ultimately decreases, stops or even reverses the venous flow5. This veno-occlusive mechanism maintains sinusoidal distention and rigid execution. A defect in this mechanism ultimately leads to vasogenic ED. Hence an attempt was made to rule out the vasogenic ED.
MATERIAL AND METHOD 40 (forty) patients of Radio-diagnosis department of Apollo Hospital, Apollo Institute of Medical Sciences and research Jubilee Hills, Hyderabad-500096, Telangana was studied. Inclusive Criteria: The patients with ED complaints referred by the urology and Medicine department. Exclusion Criteria: Who had a history of penile and/or urethral surgery and pelvic surgery, Neurological; hormonal and psychological disorders causing ED were excluded from the study. Method: Male patients having ED since the last six months and to evaluate the impotency was examined physically and psychologically. The routine investigations were carried out and patients were examined with grayscale and colour doppler sonography using an ultrasound unit with a high frequency wide 6-13 MHz linear array transducer in a quiet comfortable room to ensure privacy. Grayscale sonograms were obtained in longitudinal and transverse planes. The probe was placed longitudinally along the proximal part of the penis. Arterial diameters were measured by placing the cursor on cavernous arteries colour Doppler ultrasonography was then performed to display blood flow through the cavernous arteries. By using the colour image as a guide to the location and direction of flowing blood, the Doppler sample volume cursor was placed accurately in the cavernous arteries at the base of the penis and doppler angle correction was adjusted to match the correct axis of flow. The resulting angle corrected velocity waveform was displayed on the monitor and PSV were measured and recorded. Both cavernosal arteries were evaluated in every patient, after scanning the penis in the flaccid stage 30mg (1ml) of papaverine was injected into the corpus cavernosum by using a 26G needle. After 5 minutes (to allow uniform diffusion and physiologic response to the papaverine) scanning was performed again up to 30 minutes. Bilateral cavernosal artery diameters were measured PSV’s of cavernosal Instructions were given to patients to return to the department if the erection does not subside within 3 hours or if excess pain developed any time after injection of papaverine. Based on the results 3 intervals values were chosen 5cm/sec, 10 cm/sec and 15 cm/sec for the lowest normal pre-intracavernosal injection PSV, PPV or PSV in flaccid penis was done in predicting arteriogenic impotence as diagnosed by post-ICI doppler sonography. A PSV less than 25cm/sec, after papaverine injection associated with abnormal clinical response, was used as the diagnostic criterion for arterial insufficiency patients with suspicious venous incompetence on colour Doppler sonography were excluded from the study.
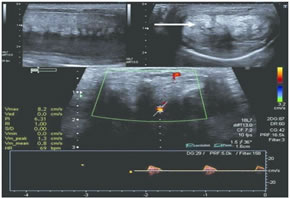
Figure 1: Penile Doppler study in a patient with significant ED
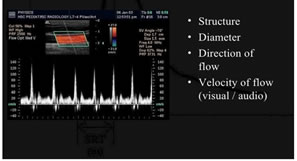
Figure 2: Color Doppler Sonography showing PSV of ED
OBSERVATION AND RESULTS Table-1: Peak systolic velocity study (PSV) highest PSV 35.1 – 45.0 was observed in 9 right cavernous artery and 11 left cavernous artery and least PSV observed in 12 patients (right and left cavernous artery) Table-2: Correlative study between PSV in cavernosal arteries in flaccid state and their clinical response after ICI – Abnormal cases were 11 (27.5%) and normal was 27 (72.5%). Table-3: Comparative study between pre and post ICI values at 5 minutes baseline sensitivity was 33.2% specificity was 100% NPV was 82.1% and PPV was 100% after 10 minutes interval sensitivity was 91.5 specificity was 92.8% NPV was 96.8 PPV was 80.9. After 15 minutes internal sensitivity was 100% specificity 18.9% NPV was 100% and PPV was 27.8%.
Table 1: Study of peak systolic velocities (PSV) in cavernosal arteries after intra-caval injection (post-ICI) of papaverine
Out of 40 patients 11 (27.5%) had abnormal clinical response, 29 (72.5%) had normal clinical response. Table 2: Correlative study between peak systolic velocity (PPV) in cavernosal arteries in flaccid state and their clinical response after IntraCavernosal injection (ICI)
Table 3: Comparative study between pre ICI and post-ICI values
NPV = Negative predictive value PPV = Positive predictive value 10 cms/sec had lowest normal PSV had best accuracy among all three values sensitivity 91.5% specificity 92.8% and PPV 80.9%
DISCUSSION The present study of ED in patients of flaccid patients using colour doppler sonography in Telangana Population – PSV was 35.1-45 was observed in 9 right and 11 left cavernous artery and least PVS observed in 12 patient (right and left correlations artery) (Table-1). In the correlative study between PSV in cavernous arteries, 11 (27.5%) were abnormal 29 (72.5%) were normal (Table-2). In the comparative study between pre and post ICI values at the interval of 10 minutes interval was 91.5% specificity was sensitivity 92.8% NPV was 96.8% PPV was 80.9% which was an ideal finding to determine the vascularity of flaccid penis (Table-3). These findings were more or less in agreement with previous studies6,7,8. Penile erection occurs with a complex interaction between neural arterial venous and sinusoidal system any defect in this system leads to ED that is a serious health dilemma affecting both men and their partners. ED scans have psychogenic organic (endocrine disorders neurogenic morphological penile abnormalities and drug-induced) or mixed aetiology (9) vascular pathology is called arterial impotence or venogenic impotence. It is also reported that sono elastography on Peyronie's plaques reveals penile lesions10 one more technique is ultrasound Vibro Elastography shows stages of erection. With papaverine injection priapism was observed in the same young patients and some have short term complications. Both arteriogenic and vasogenic ED are managed medically and surgically but the management protocol differs (11). Medical treatment involves the use of oral phosphodiesterase 5 inhibitors (PDE5i) when oral ED therapy fails intracavernosal injections, intraurethral suppositories, vacuum erection devices and penile prosthesis may be implored. Zotaro-limuseluting peripheral stents of internal Iliac Artery and Internal Pudendal artery is a treatment of option for arteriogenic ED in the presence of a proximal fixed obstruction to arterial front12 . Open surgical ligation of deep dorsal vein and its collaterals an option with variable success rates.
SUMMARY AND CONCLUSIONThe present study of ED in patients with flaccid penis using penile colour doppler sonography helps to rule out vascular insufficiency. It is a useful tool to rule out the cause of ED if vasogenic or any other cause but this study demands further angiological, pathophysiological, neuro-muscular study because exact pathogenesis of vascular ED is still unclear. This research work was approved by the Ethical committee of Apollo Hospital, Apollo Institute of Medical Sciences and research, Jubilee Hills, Hyderabad-500096. REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Radiology (Print ISSN: 2579-0927) (Online ISSN: 2636-4689) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
Height, IVDL-Intervertebral Disc Length
Policy for Articles with Open Access
Authors who publish with MedPulse International Journal of Radiology(Print ISSN: 2579-0927) (Online ISSN: 2636 - 4689) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work. |
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.