 Home
Home
|
Table of Content Volume 17 Issue 1 - Janaury 2021
Role of MDCT in the evaluation of congenital cardiac anomalies
Sruthi Babu1, Shilpa Domkundwar2*
1Junior Resident II, 2Professor & HOD, Department of Radio Diagnosis, Grant Govt Medical College and JJ Group of Hospitals Byculla Mumbai, INDIA. Email: contactsruthibabu@gmail.com
Abstract Background: Congenital heart disease(CHD) is the most common birth defect that occurs in 1/125 live births. They are generally considered to be caused by multifactorial inheritance. The factors are usually both genetic and environmental where a combination of genes from both parents, in addition to unknown environmental factors, produce the trait or condition. MDCT provides superior morphological characteristics as compared to echocardiography and catheter cardio angiography, which are limited by small field of view, acoustic windowing, and operator dependence and overlapping of adjacent vascular structures. Materials and methods: In this retrospective study, 25 patients, both male and female ranging from the age group 6 days to 60 years were included. Cardiac CT was performed on ultra fast scanner with 1 mm slice thickness and 0.75 mm collimation after intravenous administration of non-ionic contrast agent at the rate of 4.5cc/sec with trigger of 180 HU in descending aorta. Scanning was performed from the thoracic inlet level to the L1–2 level. Retrospective 3D reconstruction of data was performed to obtain volume rendered images. Results: MDCT provides superior morphological characteristics as compared to echocardiography and catheter cardio angiography, which are limited by small field of view, acoustic windowing, and operator dependence and overlapping of adjacent vascular structures. Conclusion: Considering the majority of the patients, which are children MDCT is the preferred investigation for the morphological assessment of CHD. Thin slice thickness (even 0.6mm) and short time duration of scan allows the maximum morphological knowledge. Combined Echocardiography and CT can be used to overcome the limitations of these two modalities. Systematic approach to each case can simplify the process of diagnosis without compromising the quality of reporting. Key Words: Congenital heart disease, MDCT, Cardiac CT
INTRODUCTION Congenital heart diseases (CHD) are a wide spectrum of disorders and corresponding clinical profile ranges from asymptomatic to fatal conditions. Timely diagnosis of congenital heart disease is crucial for proper management and better outcome. An array of primary cardiac imaging modalities are used for the evaluation of congenital heart diseases starting with the conventional chest radiographs to echocardiography, cardiac Computed Tomography ( Cardiac- CT) , catheter cardio angiography and cardiac Magnetic Resonance Imaging ( cardiac MRI ). Even though there are certain limitations pertaining to Cardiac CT, it is preferable modality for a wide range of CHDs.
AIMS AND OBJECTIVES MDCT provides superior morphological characteristics as compared to echocardiography and catheter cardio angiography, which are limited by small field of view, acoustic windowing, and operator dependence and overlapping of adjacent vascular structures. In this study we aimed to analyze the morphological characteristics of CHD which could be instrumental in the further management of the patient. A systematic approach to the cardiac imaging to simplify the complexity in diagnosis and satisfying the needs cardiologist/surgeon in the management with minimum affordable rate is our motive.
MATERIALS AND METHODS This retrospective study was performed in the department of Radio-diagnosis in a tertiary health care institute including 25 patients referred from pediatric and general medicine department with a variety of clinical spectrum which will be discussed further. Both male and female patients ranging from the age group 6 days to 60 years were included in this study. Patients with any absolute contraindication for contrast CT like patients with deranged renal function were excluded from the study. Cardiac CT was performed on ultra fast scanner with 1 mm slice thickness and 0.75 mm collimation after intravenous administration of non-ionic contrast agent at the rate of 4.5cc/sec with trigger of 180 HU in descending aorta. Scanning was performed from the thoracic inlet level to the L1–2 level. The intravenous contrast was administered through the lower limb preferably, whereas an arm vein was used in patients who had undergone bidirectional cavopulmonary shunting, Fontan procedure or when the lower limb vein was not accessible. Retrospective 3D reconstruction of data was performed to obtain volume rendered images.
RESULTS Age and sex distribution of patients: Out of 25 patients, there were 15 females and 10 males in this study. Female patients exceeded the number of male patients in all the age groups. 95% of these patients are below 30 years. Symptoms: Among the 25 patients studied, the most common symptom was difficulty in breathing (68%). Other symptoms include recurrent lower respiratory tract infections(36%), cyanosis (16%), chest pain (16%), hypertension, failure to thrive, giddiness and palpitations. Overlapping of symptoms was noticed in most of the patients (90%).
Table 1:
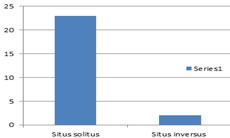
Morphological evaluation: Systematic approach was done. Viscero atrial Situs: 23 (92%) patients were with situs solitus and 2 (8%) were with situs inversus. Table 2:
Figure 1:
Ventricular Loop Orientation: In our study, out of the 25 patients 3 (12%) are showing Levo loop (L- loop) orientation and rest of them (88%) are dextro-loop (D-loop). Position and Relation of the Great Vessels: Among the study cases 14 (56%) showed normal relation (situs) of the great vessels, 6 (24%) showed transposition of great vessels and showed 2(8%) levo-malposition of great vessels and 3 (12%)showed dextro-malposition of great vessels. Ventricular septal defect: In our study, 13 (52%) patients showed ventricular septal defects. Out of which 8(66%) were membranous type. Atrial septal defect (ASD): There are four major types of atrial septal defect, that is ostium secundum, ostium primum , sinus venosus type and coronary sinus type ASD. Our study cases presented with atrial septal defects include (12, 48%). Most of them are ostium secundum type (10, 40%).
Table 3:
Figure 3:
Changes of pulmonary hypertension: In our study, 12 (48%) patients showed changes of pulmonary hypertension in the form of dilated main pulmonary artery with or without their branches dilatation. 7(28%) patients showed right ventricular and right atrial hypertrophy. Chamber status: In our study 7(28%) patients showed right ventricular and right atrial hypertrophy.2 cases showed double outlet single ventricle, 1 case with double chambered right ventricle with right atrial and right ventricular dilatation ,2 cases showed dilated RA with atrialization of RV. One case showed left sided juxta position of atrial appendages with double outlet left ventricle and hypoplastic right ventricle. The septal defects with resultant interchamber communication are already taken into account. Anomalous pulmonary venous communication: In our study there 8 patients with anomalous pulmonary venous communication (APVC). Out of this 4 were total anomalous pulmonary venous communication (TAPVC). Of these 4 patients of TAPVC, two were with supra cardiac TAPVC , one was with cardiac and one with infra cardiac type. Persistence of left superior vena cava SVC: In our study 5 (20%) cases showed persistence of left SVC. Patent ductus arteriosus (PDA): In our study 5 (20%) cases showed patent dustus arteriosus.
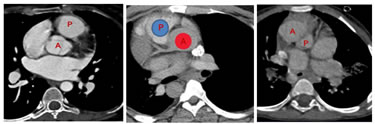
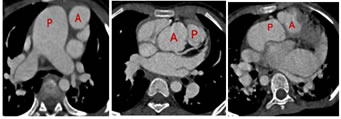
DISCUSSION With the advancement of diagnostic radiology there is undoubted positive impact on the patient management. Imaging modalities play a key role when it comes to planning the treatment /surgery. Cardiac MRI is another promising technology which allows dynamic evaluation of the heart. The time consumption of scan and the requirement of general anesthesia makes the clinician to go for CT over MRI in most cases of CHDs .The increased slice thickness and the respiratory artifacts adds the limitation of MRI in the morphological evaluation of CHD. Computed tomography (CT) has an important role in the morphological evaluation of patients with congenital heart disease (CHD). We can obtain isotropic volume data, and high-quality two- and three-dimensional multiplanar reformatted images. A systematic approach to the cardiac imaging will simplify the complexity in diagnosis without compromising the quality of reporting. The approach should start with describing the Van Praagh notation of our study cases. It is helpful for structuring the interpretation of imaging studies as well as the reporting of results. It includes Viscero atrial Situs, Ventricular Loop Orientation and Position and Relation of the Great Vessels. In normal anatomic configuration’{S, D, S}’, the first ’S' indicates that the morphologic right atrium and largest hepatic lobe are on the patient’s right and the morphologic left atrium, stomach, and spleen are on the left side (ie; situs solitus). D indicates that the ventricular loop is curved rightward (dextro- or d-loop). The last ‘S' indicates that the aorta is posterior to and rightward of the main pulmonary artery (situs solitus). The abnormality in viscero atrial situs are situs inversus and situs ambiguous. In situs inversus right atrium and largest lobe of the liver are on the left side of the patient and the morphologic left atrium, stomach, and spleen are on the right, assign the letter I for situs inversus. If the visceroatrial arrangement does not fit into either of these categories, assign the letter A to represent situs ambiguous. For determining the ventricular loop orientation, first try to identify the morphologic right and left ventricles on the basis of their intrinsic characteristics . If the morphologic right ventricle is located rightward of the morphologic left ventricle it is dextro loop (D loop). If reverse , it is levo loop (Lateral-loop). The third step is to determine the position and relation of the great vessels. In the normal configuration of the great vessels, the aorta is posterior to and rightward of the main pulmonary artery (MPA). It is designated by the letter S to denote situs solitus, “{_, _, S}” . When the aorta maintains its normal posterior relation to the MPA but has an inverted position leftward of the MPA, it is called situs inversus, designated as “{_, _, I}”. If the aorta is anterior to and rightward of the MPA, the anomaly is described as dextrotransposition, or d-transposition, of the great vessels, which is denoted as “{_, _, d-TGV}”; if the aorta is anterior to and leftward of the MPA, the anomaly is described as levotransposition (l-transposition) or congenitally corrected transposition, which is denoted as “{_, _, l-TGV}.” If the aorta is neither anterior nor posterior to the MPA, the great vessels are usually described as malpositioned. In the next step we have to look for the cardiac chambers and ventriculoarterial connection, relationship between the upper lobe bronchi and pulmonary arteries,the great vessels ( aorta, pulmonary artery, pulmonary vein), coronary artery, valves, systemic veins (superior vena cava, inferior vena cava, hepatic veins). Before going into the cases, it is important to know about the developmental anatomy of heart.In early embryonic development, the heart is a linear tube consisting of several segments that eventually give rise to the main cardiac components. Proceeding caudocephalad along this tube (from the proximal to the distal end), these segments include primitive atria, the left ventricular structure, the bulbus cordis (which will develop into the right ventricle), and the truncus arteriosus (the future great vessels) .During development, the tube bends over on itself, toward either the right or the left. Normally, the cardiogenic crescent folds to the right, forming a d-loop, with resultant positioning of the bulbus cordis to the right of the left ventricle . As the loop forms, the cephalic end of the heart tube bends ventrally, caudally, and slightly rightward to establish the spatial relationships of the future heart chambers. Figure 4: SITUS SOLITUS; SITUS INVERSUS; D-TGV
Figure 5: Lateral-TGV; D-MGV; Lateral-MGV
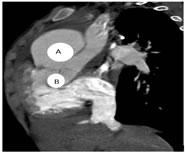
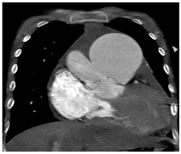
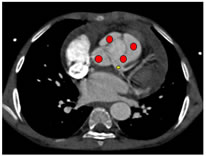
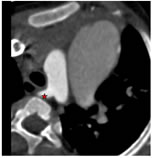
CASE 1: 10 year old child with complaints of breathlessness since birth. On ECHO cardiography Type I persistent truncus arteriosus and persistent foramen ovale was diagnosed. CT cardiac added the detailed anatomy of the common trunk and origins of the coronary arteries which is required for the pre operative planning. Van Praagh notation (S,D,S) Figure 6 Figure 7 Figure 8 Figure 6: A. Grossly dilated pulmonary trunk. B. Common trun; Figure 7: Morphological right ventricle is giving rise to a single trunk which is diving into aorta and main pulmonary artery -suggestive of Collet and Edwards Type I persistent truncus arteriosus; Figure 8: 1. The truncus shows 4 cusps with four sinuses; 2Left coronary artery arising from left posterior coronary sinus
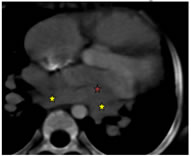
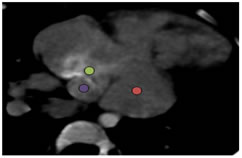
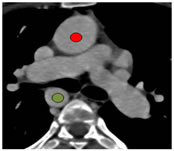
An 8-year-old female child presented with breathlessness with cyanosis and clubbing. The cardiac CT findings are shown below. Van Praagh notation (S,D,S) Figure 9 Figure 10 Figure 11 Figure 9: 1.Pulmonary veins opening into dilated coronary sinus; Figure 10: 1Ostium secundum ASD; Left atrium; Dilated coronary sinus draining into right atrium; Figure 11: Aberrant right subclavian artery
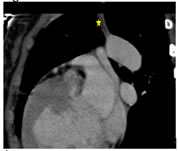
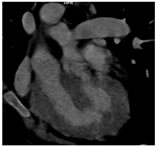
A 21 year old male presented with breathlessness on exertion and bluish discoloration of nails since 1 month. It was a known case of complex cyanotic congenital heart disease. Operated – modified Blalock Tausig shunt. Figure 12 Figure 13 Figure 14 Figure 12: Transposition of great arteries with aorta on right and anterior to pulmonary artery. Right sided aortic arch with mirror branching; Figure 13: Blocked Blalock-Taussig shunt; Figure 14: Double outlet single ventricle
CONCLUSION Considering the majority of the patients, which are children MDCT is the preferred investigation for the morphological assessment of CHD. Thin slice thickness (even 0.6mm) and short time duration of scan allows the maximum morphological knowledge. Combined Echocardiography and CT can be used to overcome the limitations of these two modalities. Systematic approach to each case can simplify the process of diagnosis without compromising the quality of reporting. The Van Praagh notation and systematic evaluation of the cardiac chambers, ventriculoarterial connection, relationship between the upper lobe bronchi and pulmonary arteries,the great vessels ( aorta, pulmonary artery, pulmonary vein), coronary artery, valves, systemic veins (superior vena cava, inferior vena cava, hepatic veins) will help to understand the anatomy and pathology.
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Radiology (Print ISSN: 2579-0927) (Online ISSN: 2636-4689) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
Height, IVDL-Intervertebral Disc Length
Policy for Articles with Open Access
Authors who publish with MedPulse International Journal of Radiology(Print ISSN: 2579-0927) (Online ISSN: 2636 - 4689) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work. |
|

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.