 Home
Home
|
Table of Content Volume 17 Issue 3 - March 2021
Role of triphasic CT in the characterization of focal liver lesions
Mahesh Kadam1, Chandrashekhar Mundkar2*
1Associate Professor, 2Assistant Professor, Department of Radiology, Vilasrao Deshmukh Government Institute of Medical Sciences, Latur, Maharashtra, INDIA. Email: mahesh2kadam@gmail.com
Abstract Background: Focal liver masses are include a variety of malignant and benign neoplasms. In cross-sectional imaging, two basic issue relate to a mass lesion: characterization of known hepatic lesion (what is it?) and detection (is it there). Commonly encountered benign hepatic lesions includes hepatic cyst, bilioma, hepatic abscess, granuloma, focal nodular hyperplasia, hepatic adenoma, bile duct adenoma, angiomyolipoma, leiomyoma, mesenchymal hamartoma and hemangiomas. Triphasic spiral computed tomography technique allows imaging of the entire liver in three phases, from the time of administration of contrast. Aims and Objectives: To study role of triple phase computed tomography in diagnosis of benign and malignant focal liver lesions. Materials and Methods: Study Site: This study was conducted at Radiodiagnosis Department. Study duration: 18 months (Data collection-12 months and analysis 6 months). Radiological Techniques: Using the mulislice(128 slice scanner) the entire liver will be scanned successively, in arterial, portal and equilibrium phases. Results: Triphasic CT of liver is a standardized CT procedure, enables in detection and characterization of vast majority of focal liver lesions, in the presence of different pathological conditions and multilevel disease. Despite increased competition from MRI over last decade, role of diagnosis of diseases of liver has not been significantly affected. Besides the general availability of the method, the dominance of CT is primarily due to its excellent visualization of anatomic relationship and of liver position relative to adjacent organs. Keywords:
INTRODUCTION The liver plays very significant role in the metabolism of carbohydrates, amino acids, lipids and synthesis of proteins. The basic pathophysiology of parenchymal hepatic diseases usually depicts an alteration in one of these metabolic pathways. Focal liver masses are include a variety of malignant and benign neoplasms. In cross-sectional imaging, two basic issue relate to a mass lesion:characterization of known hepatic lesion (what is it?) and detection (is it there). Commonly encountered benign hepatic lesions includes hepatic cyst, bilioma, hepatic abscess, granuloma, focal nodular hyperplasia, hepatic adenoma, bile duct adenoma, angiomyolipoma, leiomyoma, mesenchymal hamartoma and hemangiomas. Triphasic spiral computed tomography technique allows imaging of the entire liver in three phases, from the time of administration of contrast. The first phase is the hepatic arterial phase, which enables early identification of primary malignancy of the liver (hepatocellular carcinoma) and benign lesions (such as hemangioma, focal nodular hyperplasia and hepatocellular adenoma). The second phase is the portal venous phase, which is the most sensitive phase to detect some hypervascular tumors (hepatocellular carcinoma, metastatic melanoma, etc) and most of the hypovascular tumors of the liver such as metastatic lung carcinoma, metastatic colon cancer and metastatic breast cancer. The third phase is the hepatic venous phase also known as the delayed or equilibrium phase along with the hepatic arterial phase gives information on the vascularity of the lesion, which may further help to clarify the nature of the lesion. Hence, the purpose of the study is to characterize wide range of liver lesions using Triphasic Spiral Computed Tomograph The present study is done to study role of triple phase CT in characterization of liver lesions. AIMS AND OBJECTIVES
MATERIALS AND METHODSSTUDY SITE: This study was conducted at Radiodiagnosis Department.Study duration: 18 months (Data collection-12 months and analysis 6 months) SAMPLE SIZE:As per previous records, every month 8 to 10 patients are diagnosed as having focal liver mass on ultrasound andcomputed tomography in our department. Since study period isof 12 months so calculated sample size is 100.STUDY DESIGN:A cross sectional descriptive prospective study of patients diagnosed as having focal liver lesion on abdominal triplephase computed tomography.SOURCE OF DATAIt will include 100 patients diagnosed as having focal hepatic lesions on ultrasonography and computed tomography whichis a part of their routine clinical management and their relevant data is available.INCLUSION CRITERIAPatients who are diagnosed as having focal liver mass on ultrasonography and computed tomography between age 18 years to 70 years whose clinical data, imaging investigation reports and images are available.EXCLUSION CRITERIAPatients refusing consent to be included in the study.Contraindications for CT for eg: Pregnancy, contrast allergy.Hemodyamically unstable patientsPatients not having any focal hepatic mass.Patients having diffuse parenchymal liver lesion.RADIOLOGICAL TECHNIQUES The entire liver will be scanned successively, in arterial, portal and equilibrium phases. A 5mm collimation and 5mm/sec table speed will be used. All scans will be taken in the cranio-caudal direction and during single breath hold. After obtaining a digital scout view, unenhanced scan of the liver will be obtained.100-200 ml of 65% iodinated contrast material will be given by using a power injector at a rate of 1.5 to 2ml/sec. After 22 or 27 seconds the entire liver will be scanned in arterial phase. 22 seconds after the end of the arterial phase, the liver will be scanned in portal venous phase. The 20 second interscan delay is for the patient to rebreath and reposition the scan plane cephalad to the liver. After these two phases the third scan will be taken in the equilibrium phase,8-10 minutes after injection of contrast the images acquired in different phases will be evaluated in detail to identify lesions, classify according to age, clinical background and other imaging findings. Further the findings will be classified as benign or malignant. Unenhanced image: Useful for detection of calcification, hemorrhage, fatty infiltration, haemochromatosis, simple cyst and abscess. Contrast enhanced image: Helpful to study the pattern of enhancement: Homogenous or inhomogeneous and the degree of enhancement: Mild, moderate or intense enhancement. To study the vascularity of the lesion. To know the extent of invasion of the mass lesion. To know the tumoral spread. To determine the status of adjacent organ. To determine staging of mass and/or treatment plan. TRIPLE PHASE COMPUTED TOMOGRAPHY: Indications:
CT was interpreted by Number, nature, density (after and before contrast), and lobar distribution of the lesion was recorded. Age, sex, clinical features, location of the lesion, multiplicity, echo character/CT density and contrast enhancement will be evaluated in all cases. Data will be tabulated and analyzed. OBSERVATION AND RESULTS Table 1: Distribution of Benign/ Malignant focal liver lesions of the Total lesions (n= 274) in the patients (n = 100) studied.
Table 2: Distribution of Hypo vascular / Hyper vascular focal liver lesions of the Total lesions (n= 274) in the patients (n = 100) studied
Table 3: Distribution of Benign/Malignant Hypo vascular lesions (n = 164)
Table 3: Distribution of Benign/Malignant Hyper vascular lesions (n =110)
Table 4: Distribution of Hypo vascular lesions visualized on each phase relative to size of the lesions
PLN: plain study, HAP: hepatic arterial phase, PVP: portal venous phase. NV: not visualized, VG: visualized good, VE: visualized excellent.
Table 5: Observed enhancement patterns of 149 malignant lesions
Table 6: Observed enhancement patterns of 125 benign lesions
Table 7: Correlation of CT enhancement pattern in diagnosis of focal liver lesions with final diagnosis – an evaluation
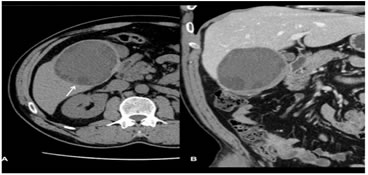
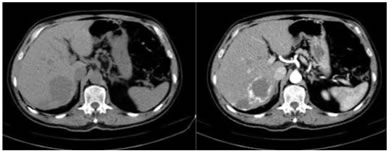
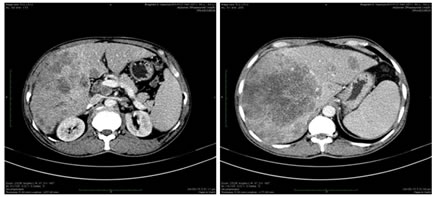
Figure 1: Multiple hyperenhancing lesions are seen through out the liver on arterial phase in known case of neuroendocrine tumor- Hypervascular metastases. Figure 2: A large well defined peripherally enhancing hypodense lesion is seen in segment V of liver- hepatic abscess. Figure 3: Few variable sized hypodense lesions are seen in segment VII of liver. They appears iso to hypodense on NCCT. On post contrast study it shows peripheral puddling of contrast in arterial phase with gradual filling in on venous and delayed phases- Hemangiomas. Figure 4: Contrast enhanced axial sections of CT abdomen shows multifocal heterogeneously enhancing lobulated soft tissue density lesions in both liver lobes – Multifocal hepatocellular carcinoma.DISCUSSIONLiver has dual blood supply (nearly 80% from portal vein and 20% from hepatic artery), most of the primary and secondary neoplastic liver lesions receive most of the blood supply from hepatic artery. During HAP hyper vascular lesions are easily identifiable against the background of minimally enhancing liver parenchyma. During PVP most of the hepatic lesions are perceived as hypo vascular lesions highlighted by strongly enhancing normal liver parenchyma. Depending upon the vascularity, a lesion will be more conspicuous during HAP or PVP.With regard to detection of lesions, in our studyOf the total 274 focal liver lesions seen in 100 patients there were 164 hypo vascular lesions accounting for 60% of the total (n=274) lesions and 110 hyper vascular lesions accounting for 40% of the total (n=274) lesions. Most hypo vascular lesions were best detected during PVP and most hyper vascular lesions in HAP. In our study a greater number of hypo vascular lesions were identified with greaterlesionconspicuityonthePVPthanonotherphasesespeciallywhenthesize of the lesion was less than 3cm in size. When the lesions size were >3cm no statistically significant difference was seen between PVP and HAP. In our study the number of hyper vascular lesions seen was higher on HAP than on PVP and unenhanced phase when the lesion size was less than 3cm in size. Significant difference in conspicuity was identified between the HAP and other phases when the lesion size was less than 3cm but no when the lesion size was greater than 3cm in size. In our study unenhanced scan had lower sensitivity for identification of small lesions because of difficulty in differentiating it from unenhanced vessels and biliary dilatation. Most of the differences were seen when the lesion size was less than 3cm, because larger lesions were seen on all phases. No patient in our study had a lesion that was detected on unenhanced phase images that was not identified on with HAP or PVP images. In characterization of hypo vascular lesions the first distinction was madebetween cysts and hypo vascular solid lesions. All the 51(100%) lesions with hypo/hypo (cyst)/hypo enhancement pattern were confirmed to be cysts because of sharp margins and homogenous hypo vascular pattern. 15 of the 51 cystic lesions were hydatid cysts seen in 2 patients(in addition to the cystic enhancing patterns these lesions showed subtle areas of peripheral rim calcification with thin enhancing septaewithin). When enhancing rim was observed, with hyper(rim)/hypo(cyst)/hypo enhancing pattern, all the lesions (11 of 11) were abscess. In noncystic hypo vascular lesions, when the lesions demonstrated hypo/hypo/hypo enhancing pattern, 68(95.7%) of 71lesions were metastases and 3(4.3%) of 71 lesions were hemangioma (atypical). when an enhancing rim in arterial phase was observed with hyper(rim)/hypo/hypo pattern, all the lesions (27of 27) were metastases. hypo/hypo/hyper enhancing pattern, was seen in 4 lesions, 3(75%) were metastases and 1(25%) washemangioma. In characterization of hyper vascular lesions: All the 54(100%) lesions with A(puddles)/A/A enhancement pattern were hemangiomas. The second group of hyper vascular lesions demonstrated non specific, hyper/A/A enhancement pattern found in both malignant and benign lesions. Most (73.7%) of the malignant hyper/A/A lesions were metastases and rest of the lesions (15.9%) were HCC. The benign lesions were FNH (5.2%) and Adenoma(5.2%). With mixed/mixed/mixed enhancement pattern, all the lesions (16 of 16) were metastases. 16 of 19 HCC presented as A(variegated)/A/A(delayed), enhancing pattern.
CONCLUSION AND SUMMARYIn 100 patients total of 274 focal liver lesions were detected. 149 lesions were malignant and 125 lesions were benign. The most common malignant lesion was Metastases (n=128) followed by HCC (n=19) and Intrahepatic CCA (n=1). The most common benign lesion was Hemangiomas (n=58), followed by Cysts (n=51), Abscesses (n=11), FNH (n=4) and adenoma(n=1). Total focal liver lesions were broadly grouped into, hypo vascular or hyper vascular lesions, based on the enhancing pattern of the individuallesions. There were 164 hypo vascular lesions accounting for 60% of the total (n=274) lesions and 110 hyper vascular lesions accounting for 40% of the total (n=274) lesions. The PVP images acquired at the peak of liver enhancement is essential for detection of hypo vascularlesions. HAP images are helpful in detecting hyper vascular lesions and are essential for characterization of large proportions of lesions. Equilibrium phase images aid in further lesioncharacterization Characterization of focal liver lesions based on the 11 enhancement patterns observed and correlation with standard of reference was satisfactory. The Triphasic CT enhancement patterns were 100% sensitive and specific in diagnosing all cases of Abscess, Cysts and Intrahepatic CCA, however Triphasic CT enhancement patterns in HCC (sensitivity-84.3%), Hemangioma (sensitivity- 93.0%),FNH(sensitivity-75%),Metastases(sensitivity-97.6%)wassensitivein diagnosing most of the cases and showed 100% specificity in diagnosing in all the cases when there was typical enhancement pattern for the individual lesion concerned. Four enhancement pattern observed were always due to benign lesion. Four more enhancement pattern observed was always due to malignant lesion. The hypo/hypo/hypo, hypo/hypo/hyper and hyper/A/A enhancement patterns need to be interpreted with caution. Few of the limitations in our study are; lesion by lesion pathological evaluation was not performed; in defining CT pattern of enhancement an objective criteria is taken into consideration; in some patients with multiple lesions, biopsy was performed on only two lesions, rest with similar CT appearance were assumed to be the same lesion; technical factors like amount of contrast injected, concentration of the contrast and physiological status of the patients. Triphasic CT of liver is a standardized CT procedure, enables in detection and characterization of vast majority of focal liver lesions, in the presence of different pathological conditions and multilevel disease. Despite increased competition from MRI over last decade, role of diagnosis of diseases of liver has not been significantly affected. Besides the general availability of the method, the dominance of CT is primarily due to its excellent visualization of anatomic relationship and of liver position relative to adjacent organs. REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Radiology (Print ISSN: 2579-0927) (Online ISSN: 2636-4689) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
Height, IVDL-Intervertebral Disc Length
Policy for Articles with Open Access
Authors who publish with MedPulse International Journal of Radiology(Print ISSN: 2579-0927) (Online ISSN: 2636 - 4689) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work. |
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.