 Home
Home
|
Table of Content - Volume 19 Issue 3 - September 2021
Triple culture as a guide for predicting post-percutaneous nephrolithotomy systemic inflammatory response - A Prospective Study
Sivasankar M1, Griffin M2*, Dev Krishna Bharathi C3, Basudev Kumar Jha4, V Kamaraj5, Muthulatha N6
1,5,6Professor, 2Associate Professor, 3Assistant Professor, 4Senior Resident, Department of Urology, Saveetha Medical College Hospital, Chennai, INDIA. Email: aureliusgriffin@gmail.com
Abstract Background: Systemic inflammatory response due to manipulation during percutaneous nephrolithotomy can beholocaust despite prophylactic antibiotic and negative midstream urine culture. It is well known that bacterial flora of stone when manipulated during surgery can cause sepsis post surgery due to release of bacterial toxins and colonisation so stone culture and renal pelvic fluid culture can guide to postoperative urosepsis and SIRS management and patient recovery. In this prospective study we determined the importance of triple culture ie, preoperative urine, renal pelvic fluid and stone crush culture a guide to post operative SIRS. All patient fulfilling the selection criteria for PCNL underwent triple culture and patient monitored for post operative systemic inflammatory and statistically analysed. A total of 50 patient under went analysis of which mid stream urine culture were positive in 18% of case, 32% were positive for stone crush culture, and 26% were positive for pelvic fluid culture. out of which stone crush culture sensitivity for SIRS were 75%, renal pelvic fluid culture sensitivity for SIRS were 61.5%, and preoperative urine culture sensitivity was 52.5%. and relative risk for predicting SIRS with stone crush culture and renal pelvic fluid was more than twice the pre-operative midstream urine culture and p value was statistically significant. Result of this study suggest that stone crush culture and renal pelvic fluid culture are better predictor of post PCNL SIRS then preoperative midstream urine culture. Keywords: Systemic Inflammatory Response Syndrome, Percutaneous Nephrolithotomy, Renal Pelvic Urine Culture
INTRODUCTION Percutaneous nephrolithotomy is the most preferred intrarenal surgery for large renal stone, and septicemia occurring post-surgery is quiet devastating and challenging in health care system despite pre-operative urine culture remaining sterile and prophylactic antibiotics and can trigger systemic inflammatory response post operatively.1,2 patients with a sterile pre-operative urine culture can develop post-operative sepsis after stone manipulation or fragmentation possibly because of release of bacteria in blood stream.3,4 This can also result in progress to multi-organ failure and even death if not managed promptly and aggressively. Thus, urosepsis in post-operative period may prove to be catastrophic despite adequate pre-operative antibiotic coverage, and negative urine culture. Bacterial flora of the stone and pelvic fluid thus can help and guide for treatment and prevention of post-operative urosepsis or systemic inflammatory response syndrome. Intraoperative Stone crush culture and pelvic fluid culture is not a routine practice during Percutaneous nephrolithotomy and preoperative urine culture is heavily relied upon for post-operative sepsis or systemic inflammatory response complication. Thus aim of my study is to find correlation and significance of intraoperative pelvic fluid and stone crush culture can be used as a surrogate marker for stone bacterial flora. METHODS This non-randomized observational study was conducted from September 2019 to October 2020.In this study, we ana- lysed culture specimens, namely midstream urine (MSU), intraoperative pelvic fluid culture and stones crush culture of 50 patients during PCNL. Exclusion criteria: Patients with urogenital malignancy. Patients with others causes of sepsis. Severely immune compromised patients (diabetes, HIV, etc.) Patients already on broad spectrum antibiotic before urine culture. Patients on steroids. Patients with congenital urologic anatomical anomalies. Patients on prolonged catheterization or stents. All patient underwent midstream urine culture evaluation 14 days before surgery. Based on urine culture result all negative patient was given a preoperative dose of prophylactic intravenous broad- spectrum antibiotics, which were then continued for 24 hours postoperatively. For culture positive (greater than 10,000 cfu/ml), the patient received a minimum 7-day course of oral antibiotics based on the sensitivity profile, and continued until the day of surgery. The procedure involved initial cystoscopic placement of an open-ended catheter in the ipsilateral ureter with the patient under general anesthesia Renal pelvic urine was collected via retrograde ureteral catheter placement or during percutaneous puncture of the pelvicalyceal system. The retrieved fragmented stones was rinsed in 0.9% normal saline, crushed and sent in a sterile tube for microbiological evaluation. Postoperatively patients were closely monitored for signs of systemic inflammatory response, which is characterized by 2 or more of certain conditions, including 1) body temperature less than 36C or greater than 38C, 2) heart rate greater than 100 beats per minute, 3) respiratory rate greater than 20 breaths per minute and/or 4) leukocyte count greater than 12,000 white blood cells per micro lt or fewer than 4,000 white blood cells per micro ll. The collected data were divided into 3 main groups, that is MSU CandS, pelvic CandS (urine proximal to the obstructing stone) and stone CandS. We performed statistical analysis of the data obtained using the Fisher exact and Mantel-Haenszel chi-square tests to determine associations among the various groups and subgroups. The t test was used to compare mean stone size among the subgroups analyzed. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and association risks were calculated.
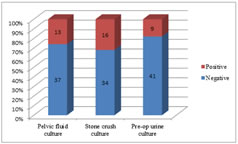
RESULTS Of the 50 cases enrolled in this study, 32 (64%) were male and 18 (36%) were female (M/F ratio was 1.9:1) with mean age of 50.32 years. All patients were divided into 3 groups according to the site of culture specimen. Among the study population, 18% had a positive pre-operative urine culture, whereas 32 % patients were positive for stone culture and 26% were positive for pelvic fluid culture (fig 2).
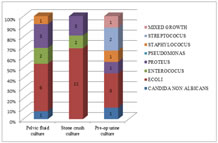
Table 1: Patient and stone demographics Most common bacteria isolated in pre-operative urine culture were E. Coli (33%), followed by streptococcus (22%), while The most common bacteria isolated in stone crush culture was E.coli (68%) followed byproteus (18.75%), and in pelvic fluid culture the most common organism is E. coli (46%) followed by proteus (23.07%) .
Figure 1: Type of microorganism cultured Figure 2: Culture positive specimen
On comparing the result of bacteriological analysis of stone crush culture, urine culture and pelvic fluid culture, it was seen that only 5 (10%) patients were positive for both stone and urine culture, while all 3 specimens were simultaneously culture positive in 1 patient (2%). Preoperative urine culture determining infected upper urinary tract had PPV,NPV and relative risk of 0.5, 0.6and 1.20 respectively. We noted a post procedural systemic inflammatory response (SIRS) in 16 patients (32%) of which 14 had at least 1 culture positive. None had positive blood culture. Stone crush culture and pelvic fluid culture carried more than twofold risk of systemic inflammatory response on correlation between various specimen. Sensitivity and Specificity of stone crush culture for predicting systemic inflammatory response are 75%,and 88% respectively, while Sensitivity and Specificity of pelvic fluid for predicting systemic inflammatory response are 61.54% and 78.3% and Sensitivity and Specificity of pre-operative urine culture were 52.56% ,62.50% respectively. The positive predictive value of pre-operative urine culture, stone crush culture and pelvic fluid culture were 31.2%,75%and 60% respectively (tab 2). While the P value of stone crush culture specimen were <0.001, pelvic fluid were 0.001 and pre-operative urine culture were 0.377 which was not significant.
Table 2: Predicting SIRS using various specimens
There was a poor correlation between SIRS and age (p = 0.56), sex (p = 0.34), difficult access (p = 0.803) and residual stones postoperatively (p =0.697). Stones were found to be larger in infected system then non infected system. However, the pooled 2-tailed t test revealed no statistical difference in the mean bulk of infected and non-infected stones (t = 1.463, p = 0.151).
DISCUSSION During preparation for percutaneous nephrolithotomy it is common practice to culture preoperative midstream urine a week before surgery and render patient sterile with appropriate antibiotics for 7-10 days and then urine C and S was repeated. Antibiotics prophylaxis has been done in accordance with European Association of Urology (modified from Infectious Diseases Society of America, and European Society of Clinical Microbiology and infectious diseases) guidelines.5 However even after careful preoperative care Urosepsis and SIRS tends to occur as preoperative urine culture does not always indicate infected renal pelvic fluid and stone culture in patient with sterile midstream urine culture. One prospective study done by Mariappan et al. 54 patients undergoing PCNL were evaluated with preoperative midstream, stone and renal pelvic culture.6 PBUC was positive in 11.1% of patient while SC and RPUC were positive in 35.2% and 20.4%, respectively. Only 3 patients (5.6%) had positive PBUC with positive SC and/or RPUC. In another report positive SC was associated with sterile PBUC in 19 of 75 patients (25%).7 In that study the sensitivity of urine culture to detect positive SC was only 30%, although specificity was significantly higher at 94%. In our study we also came to conclusion about need of upper tract culture during percutaneous nephrolithotomy to prevent post-operative sepsis and Systemic inflammatory response eight of the 13 patients (61%) with positive renal pelvic fluid culture had a negative pre-operative urine culture while Twelve of the 16 patients (75%) had negative pre-operative urine culture. This was also seen in one of the prospective randomized study done by Korets et al. 204 patients underwent PCNL were evaluated with PBUC, RPUC and SC.8 In the study 33% of the patient with positive RPUC had negative pre-operative urine culture, while 48.5% with positive SC had negative pre-operative urine culture. Main challenge lies in predicting Systemic inflammatory response post PCNL in patient with negative pre-operative urine cultur.1,2 Stone crush culture and renal pelvic fluid culture is reliable in predicting Systemic inflammatory response. In one of the retrospective study of 338 patients who underwent PCNL 82 (24.2%) had postoperative fever, which progressed to sepsis in 5 (1.5%).9 Out of 82 patients with SIRS 66% of patient were having negative urine culture and remaining 34% with positive culture were treated with culture sensitive specific antibiotics till urine culture grew no bacteria. Another Prospective study of 75 consecutive patient preoperative urine culture was not significantly associated with SIRS.7 In my study similar correlation with previous study was noted and conclusion was made that preoperative urine culture is not a predictive of Systemic inflammatory response and we came to opinion that preoperative urine culture should be done and treated accordingly till culture become negative and neither positive nor negative preoperative urine culture is predictor of Systemic inflammatory response. One of the Report by Dogan et al. 57.3% of patient with Post PCNL SIRS had positive SC compared to 26.6% who did nothave.9 Margel et al. found that SC had 3.6 relative risk for SIRS.7 Several factors have been identified as risk for post-PCNL fever and sepsis including age, stone size, female gender, paraplegia.5,10,11,12,13We found no statistically significance in age ,gender and in our study stone bulk did not correlate with systemic inflammatory response although larger stones were infected . we generally believed that larger stones are more likely to harbor bacteria and are generally infectious stone. Study by Cadeddu et al. suggested no correlation between stone composition and post-operative fever.14 To our knowledge there is no literature available that attempt to correlate age, sex, residual stones and SIRS in index Medicus. We believe that patients with Post PCNL SIRS, upper tract culture will guide to better antibiotic use for speedy recovery.
CONCLUSIONS We came to conclusion based on our study that patient undergoing Percutaneous nephrolithotomy should undergo stone crush culture and pelvic fluid culture as there are better predictor of sepsis or systemic inflammatory response syndrome then preoperative midstream urine culture, as it helps in better guide to antibiotic use and fasten the recovery of sick patient.
REFERENCES
Policy for Articles with Open Access
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.