 Home
Home
|
Table of Content - Volume 20 Issue 1 - October 2021
A rare case of giant loose peritoneal body - A diagnostic dilemma
Maheshkumar Soni1, Prasad Upganlawar2, Akash Mahalle3, Kshitij Arun Mane4*, Atuf Muqri5, Jyoti Bhondekar6, Mahendra Pawar7
1Associate Professor, 2Assitant Professor, 4,5,6,7Resident Doctor, Department of General Surgery, Government Medical College, Nagpur, Maharashtra, INDIA. 3 Director, Spectrum imaging centre, Dhantoli, Nagpur, Maharashtra, INDIA. Email: drmaheshkumarsoni@gmail.com, drprasadupg@gmail.com, maneboy181@gmail.com
Abstract Background: Occurrence of loose peritoneal body has been known for hundreds of years. They named as Giant loose peritoneal body when they attained size of more than 5cm. It presents with very atypical and vague clinical presentation with unusual radiological findings which makes it one of the rare differentials. Thus, it should be kept as a differential along with GIST, dermoid cyst, tubercular granuloma, calcified lymph node when patient presenting with chronic vague dull aching and intermittently colicky pain associated with typical radiological finding that it changes its location as per patient’s posture or sometime during the course of presentation. In our case it is 70-year-old man presenting with chronic vague abdominal complaints which on through clinical and radiological evaluation with further operative intervention revealed as a case of Giant loose peritoneal body.
INTRODUCTION 70-year-old male presented with complaints of abdominal pain in right upper and lower quadrant of abdomen since 7 to 8 months. History of dull aching type of pain in right upper and lower quadrant non progressive non radiating and with altering location with respect to body posture, on lying down position patient complains pain in epigastric region while on standing he complains pain in lower abdomen. As per history given by patient there was intermittent episode of colicky pain throughout course of presenting complaints. Also, he added there was history of intermittent feeling of difficulty in voiding urine. There was no history of abdominal distension, altered bowel habits, melena, hematemesis, any previous operative intervention, no past history of any chronic health issue. Patient is non diabetic and non-hypertensive. All vital parameters of patients were within normal limits. Per abdomen examination suggestive of soft non tender and non-rigid abdomen, no evidence of any palpable mass in all quadrants of abdomen with normal per rectal findings. On evaluation all blood investigations was satisfactory. On radiological evaluation x ray of erect abdomen was not suggestive of any acute abdominal condition. USG revealed a large predominantly calcified mobile lesion in the pelvis with central hyper echoic dense calcific focus and surrounding alternate soft tissue area. Lesion was separated from surrounding vital structure with maintaining fat planes. CECT report revealed a well-defined solid isodense lesion measuring 4.5x4.4x4.7cm in central part of mesentry without post contrast enhancement. Bowel loops, other visceral organs surrounding to lesion found to be normal. CT took forward possibilities of benign neoplasm like solitary fibrous tumor, dermoid, GIST. Figure 1 Figure 2
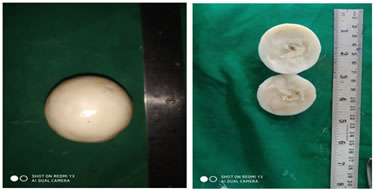
Patient was taken to OT, on midline exploratory laparotomy it was found that all internal viscera was normal. Stomach, small bowel from DJ to IC junction was traced found to be normal without any palpatory mass or any growth. Mesentry and greater momentum examined, was also found to be normal without any adhesions or any other pathological abnormality. There was a smooth rounded firm to hard white freely mobile mass found in pelvic region just right to the urinary bladder not attached to surrounding. Mass was freely and easily taken out from the pelvis whole procedure was uneventful and patient recovered well post operatively. On HPE of specimen finding suggestive of it was firm to hard a smooth rounded mass of size 5.5x5cm on cut section there was yellow fat necrosis in the centre surrounded with white multiple lamellated membranous structure appearing like cut boiled egg. microscopic examination revelled a central nidus of adipose tissue with mild chronic inflammatory infiltrate and calcifications. The adipose tissue shows fat necrosis. It is surrounded by layers of collagenous tissues. no atypical cells and no granuloma.
Figure 3 DISCUSSION A giant intraperitoneal loose body is a rare entity was known to us since long, in literature it was first reported by Littre in 1703 and its pathogenesis was first explained by Virchows in 1863 and then after by Paterson in 1933. As per Virchows, obesity or recurrent intra-abdominal infection lead to increase in fat deposition over appendices epiplocae leading slow and progressive occlusion of their blood supply making them devascularised over period of time. This ultimately lead to detachment from their parent structure and fall into peritoneal cavity freely. Paterson proposed that recurrent inflammation and torsion of base of appendix epiploecae are the main factors lead to their detachment. Fat gets calcified and sapponified over the detached appendix epiploecae along with this, over years of progression serum from peritoneal cavity get deposited over it making it progressively enlarging body. This explains the gross appearance of GLIPB , centrally presented with yellow fat necrosis of appendix epiploecae surrounded by laminated fibrinoid material.1,2,3 It has been reported that giant intraperitoneal loose body is having wide spectrum of presentation from totally asymptomatic patient in whom it reveled accidentally on laparotomy for other causes to a symptomatic acute presentation of any abdominal condition like acute abdominal obstruction this is because of varying size of loose peritoneal body . It is rare that loose peritoneal body attained size more than 5 cm so these are then termed Giant loose intraperitoneal body. Patients with GLIPB presented with vague dull aching type of pain which may or may not be localise in nature or sometimes it is presented with its altering location. Depending on its location patients presents with symptoms of nausea, constipation, intermittent colicky type of pain, dysuria, strangury, heaviness in lower abdomen. From reported cases in literature mean time period from symptom to diagnosis of condition is about 814 days (3 days to 20 years). And its presentation seen in mean age group of 56.3 years (2 months to 79 years).4,5,6,7 Though the intraoperative findings and HPE are the tool for confirm diagnosis for peritoneal loose body, radiological tools help to differentiate between other possible differential diagnosis. Peritoneal loose body should be differentiated from desmoid tumor, teratoma, calcification of lymph node, metastatic lesion of ovarian cancer, leiyomyoma, GIST, or retained sponge. With help of radiological tools it is found that there are some characteristics features of Loose peritoneal body. On plain radiological films there is e/o centrally calcified lesion which changes position evidenced by serially taken films on different position and time. On cect there is non enhancing homogenous lesion with central calcification and peripheral concentric soft tissue. Non enhancing and homogenous nature suggestive that growth / mass is free of any vascular supply. The characteristic mobile nature of Loose peritoneal body can be evaluated with CT cuts in prone position and at different time. In magnetic resonance imaging it presents as round to oval well circumscribed hypointense mass on both T1 T2 weighted image and may hyper intensed on T1 weighted due to central calcification.8,9,10,11,12 In our case there was 5.5x5 cm sized Loose peritoneal body which turned out to be Giant loose peritoneal body which typically presented with chronic vague abdominal pain without any classic clinical findings which clinches any specific diagnosis for the patient. The condition was came into picture after the radiologicalm evaluation which is the modality for the diagnosis and help to differentiate from other possible condition but HPE is the ultimate tool of the diagnosis of Giant loose peritoneal body. In our study also Loose peritoneal body presented with centrally calcified homogenous non enhancing lesion which changes its position according to the posture of the patient. HPE typically s/o centrally present yellow fat necrosis surrounded with collagenous tissue. Operative modality was the only treatment for this condition. Diagnostic laparoscopy followed by definitive procedure would be more justifiable approach for such rare entity.
CONCLUSION Loose peritoneal body being rare entity and cases of Giant loose intraperitoneal body have been documented in the literature and there is uncertainty on their developmental hypothesis. Pre –operative diagnosis of this is difficult but presentation with vague chronic abdominal complaints with or without alteration in bowl and bladder habits associated with some characteristics radiological features like centrally calcified homogenous non enhancing lesion in abdomen which may or may not changes its location according to patient posture or during the course of presentation so the rare possibility of Loose peritoneal body should be kept in mind. Diagnostic laparoscopy would be the justifiable approach for the diagnosis of such rare entity before doing exploratory laparotomy in well-established setups. No specific treatment needed in asymptomatic patients but when associated with complication or when diagnosis is in doubt exploratory laparotomy is the only treatment modality.
REFRENCES
Policy for Articles with Open Access
|
|

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.